Please have any pathology or radiology tests competed if requested during your appointment. Take your normal medications unless told otherwise by Dr Murray or the anaesthetist. Most blood thinners, with the exception of Aspirin, will need to be ceased beforehand. The procedure requires a general or spinal anaesthetic therefore you will need to fast for six hours prior.
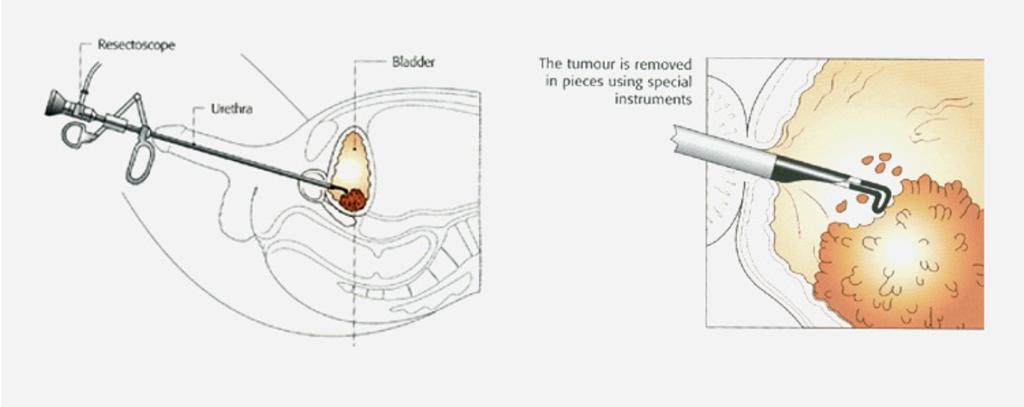
After administration of the anaesthetic the tip of the resectoscope is inserted into the urethra and advanced into the bladder. The internal lining of the bladder is visualized, and any tumours removed. Any significant bleeding is controlled using diathermy and a urinary catheter is placed.
A short period of time is required in the recovery room while the anaesthetic wears off. The catheter is connected to irrigating fluid and a drainage bag. The irrigating fluid washes away blood and prevents blood clots forming and blocking the catheter outflow. You should expect some blood in the catheter urine bag, and this will clear up in time.
You will have discomfort in the bladder (and at the tip of the penis in men) as well as a sensation of bladder fullness and the desire to pass urine. This is due to the catheter stimulating the inside of the bladder. These symptoms will settle after the catheter is removed and the bladder heals.
The catheter is usually removed by a nurse one or two days after the procedure. The nurse will measure the volume of urine passed and scan your bladder to assess the volume remaining inside. The nurse will update Dr Murray by phone and if you are emptying your bladder satisfactorily you will be discharged (usually around midday).
The bladder needs to heal after the procedure, and this usually takes one to two weeks. During this time, you should expect a stinging or burning sensation when you pass urine, the need to pass urine frequently, an urgent need to urinate and intermittent bleeding in the urine. Taking Ural sachets and paracetamol often helps. In cases of heavy bleeding with clots and an inability to pass urine you will need to present to your local emergency department as a catheter may be required.
A follow up appointment with Dr Murray will be made one to two post procedure where your pathology results will be discussed. Bladder tumours are often cancerous and additional treatments may be required; these will be discussed in detail at your follow up appointment.
Although major complications from TURBT are rare there are some important things you need to be aware of. Risks and complications include but are not limited to:
1. Haematuria (blood in the urine) and the potential need for catheter re-insertion
2. Dysuria (stinging sensation when voiding)
3. Urinary tract infection (approx. 5% risk)
4. Ureteric injury and the need for a ureteric stent or further surgery to repair
5. Bladder perforation requiring prolonged catheter insertion or further to surgery to repair
6. Stricture formation (urethral scarring causing reduction in urine flow)